Incomplete abortion is the expulsion of a portion of the conception before the gestational age reaches 20 weeks.
Abortion, also known as miscarriage, is the spontaneous termination of a pregnancy before the 20th week. Approximately 10-20 percent of pregnancies end in miscarriage. However, the actual rate is likely much higher because many miscarriages occur very early in pregnancy—even before a woman is aware of being pregnant.
Based on the timing of occurrence, miscarriages are categorized as:
Early miscarriage: Occurring at a gestational age of less than 13 weeks or 12 weeks and 6 days. Early miscarriages are the most common.
Late miscarriage: Occurring at a gestational age of more than 13 weeks.
What is incomplete abortion?
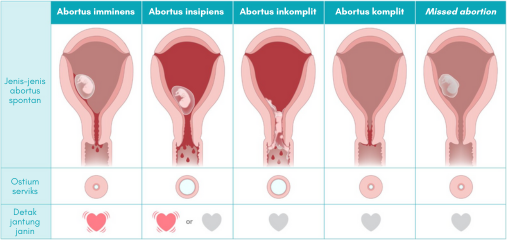
Incomplete abortion is one type of spontaneous abortion. Other types of spontaneous abortion include imminent abortion, ongoing abortion, complete abortion, and missed abortion.
Women who experience abortion typically present with complaints of vaginal bleeding accompanied by pain or cramping in the lower abdomen before reaching 20 weeks of gestation. In incomplete abortion, a portion of the products of conception (fetal tissue) is expelled along with the vaginal bleeding. On the other hand, in complete abortion, the products of conception are fully expelled.
Mulai Promil Sekarang
Another type, called imminent abortion, refers to a threatened miscarriage where there is vaginal bleeding without the expulsion of the products of conception. In this case, the pregnancy can still continue because the fetus is intact, alive, and the birth canal is not yet open. The continuation of this condition leads to ongoing abortion. In its true sense, this is an inevitable miscarriage. The fetus is still inside the uterus and alive, but the birth canal is open, resulting in an eventual miscarriage.
Sometimes, the fetus has already died but remains in the uterus. This condition is known as missed abortion. To better understand the differences between these terms, let’s refer to the diagram below.
There is a misconception that incomplete abortion is an ongoing pregnancy that has not fully ended. However, in reality, the pregnancy has already come to an end. It’s just that the fetus and related tissues have not completely been expelled. If left untreated, this condition can develop into a serious infection.
Symptoms of incomplete abortion:
The majority of miscarriages occur before reaching 13 weeks of gestation. The symptoms and signs may include:
Vaginal spotting or bleeding: Vaginal bleeding that is more than one pad per hour indicates heavy bleeding and requires immediate medical attention. The presence of large blood clots also indicates heavy bleeding.
Lower abdominal pain or cramping: Women may experience pain or cramping in the lower abdomen and/or pelvic area, which can radiate to the lower back, buttocks, genitals, and perineum (the area between the vagina and anus). The cramps may be rhythmic, similar to labor contractions, but with lesser intensity.
Passage of fluid or tissue from the vagina: Vaginal spotting or bleeding in the first trimester does not always indicate a miscarriage. In many women who experience it, the pregnancy continues until delivery time.
Causes and risk factors of incomplete abortion:
Many women may blame themselves when a miscarriage occurs. However, in most cases, miscarriage is not related to anything they have done or not done.
In general, the occurrence of incomplete abortion cannot be prevented. Fifty percent of cases are caused by spontaneous, non-inherited chromosomal abnormalities. Other factors and risk factors that can be modified contribute to the remaining cases, such as:
Maternal age: Women who are pregnant over the age of 35 are at a higher risk of miscarriage compared to younger women. At age 35, the risk of miscarriage is around 20 percent. At age 40, it increases to 40 percent. And at age 45, it rises to 80 percent.
Previous history of miscarriage: Women who have experienced two or more consecutive miscarriages are at a higher risk of miscarriage in subsequent pregnancies.
Poorly managed medical conditions: Conditions such as diabetes, hypertension, kidney disease, thyroid disease, polycystic ovary syndrome, lupus, and thrombophilia can increase the risk of miscarriage.
Infections: Infections such as HIV, sexually transmitted infections, and Listeria monocytogenes bacterial infection.
Uterine or cervical abnormalities: Certain uterine abnormalities or a weak cervix (incompetent cervix) increase a woman’s risk of miscarriage.
Risky behaviors: Risky behaviors such as smoking, alcohol consumption, and illicit drug use can increase the risk of miscarriage.
Weight: Both underweight and overweight are associated with an increased risk of miscarriage.
Undergoing invasive prenatal testing: Procedures such as chorionic villus sampling or amniocentesis carry a small risk of miscarriage.
The above factors can contribute to congenital abnormalities in the fetus, which can subsequently lead to incomplete abortion.
It’s also important to note that the following factors do not cause miscarriage:
Exercise, including jogging and cycling.
Sexual intercourse.
Working, as long as there is no exposure to harmful chemicals or radiation.
Diagnosis of incomplete abortion:
Diagnosis of incomplete abortion:
To diagnose incomplete abortion, the doctor will conduct a thorough interview regarding the occurrence of the abortion, medical history, and any potential risk factors. The woman needs to provide detailed information about her last menstrual cycle, estimated due date, as well as the history of the pregnancy and prenatal care at that time. All of this information is important because the further along the pregnancy is, the greater the risk of complications from the miscarriage, and the treatment options may differ. It is also important to know the amount of blood loss, the presence of active bleeding during the examination, and whether there is any tissue or blood clots being passed.
In almost all cases of incomplete abortion, a pelvic physical examination will reveal an open cervix (cervical os) with visible products of conception (fetal tissue). Some of the tissue may be seen protruding from the vaginal canal. In rare cases, the cervical os may be closed, but fragments of the conception can still be visible.
The ideal method to diagnose incomplete abortion is the measurement of beta-human chorionic gonadotropin (beta-hCG) hormone levels along with abdominal or transvaginal ultrasound (USG). The beta-hCG hormone levels will be low, and the ultrasound results usually show the presence of remaining products of conception in the uterus with no fetal heartbeats detected. Physical examination of the uterus, known as bimanual palpation, will reveal an enlarged uterus with a soft consistency.
Other examinations that may be performed in cases of incomplete abortion include complete blood count, blood typing, and cross-matching for blood transfusion purposes, Rh factor, and coagulation profile.
Managing incomplete abortion:
Incomplete abortion is commonly managed through expectant management, which involves close monitoring and serial beta-hCG level measurements by frequent visits to the obstetrician. In most cases, the remaining products of conception will be expelled naturally without the need for specific medications or surgery. This process can occur soon after symptoms start and may continue for several weeks.
In cases of incomplete abortion with heavy bleeding, intravenous fluid administration, pain relief medication, and blood transfusion may be necessary. Women need to be hospitalized because the bleeding is ongoing and significant, which can potentially lead to shock. Additionally, there is a possibility of removing the remaining products of conception through surgery.
When the products of conception are in the birth canal, the healthcare provider may use medical instruments to remove them. This procedure is necessary to stop the bleeding and prevent shock.
Some cases of incomplete abortion are managed with the administration of oxytocin to control bleeding and misoprostol to help the uterus contract and expel the remaining products of conception. Women may be advised to stay in the hospital until all the products of conception have been expelled or they may be allowed to go home.
Another treatment option is surgical intervention through dilation and curettage (D&C). This minor surgery is performed in the operating room under general anesthesia. This method is recommended when incomplete abortion causes severe bleeding and pain, and when signs of infection are present. Alternatively, if previous treatments such as expectant management and medications have not successfully cleared the remaining products of conception.
Complications of incomplete abortion:
The most common complication of incomplete abortion is infection in the uterus. This condition, known as septic abortion, presents symptoms such as fever, chills, lower abdominal pain, and foul-smelling discharge from the vagina.
Infection is secondary to the retained products of conception and can be caused by various bacteria. The most common ones are genital flora, such as Group B Streptococcus, B. fragilis, and E. coli. The good news is that the incidence of infection due to incomplete abortion is relatively low.
Other complications are related to the treatment of incomplete abortion. These include death, uterine rupture, uterine perforation, hysterectomy (removal of the uterus), organ failure, pelvic infection, cervical damage, vomiting, diarrhea, infertility, and psychological impact.
Conclusion
It is not easy for couples to accept the occurrence of incomplete abortion or miscarriage with an open heart. To some extent, this event inevitably has negative impacts on their emotions and psychological well-being. The good news is that incomplete abortion can be successfully managed with a success rate of up to 96 percent without affecting fertility. Women can conceive again once they resume ovulation, which can occur within two weeks after the miscarriage.
However, it is recommended for couples to wait for at least 2-3 months before attempting to conceive again after a miscarriage. This is to ensure that the woman’s reproductive organs have fully healed and are ready and optimal for the next pregnancy.
Jadwalkan Konsultasi
If you have not become pregnant after one year of marriage, we recommend that you undergo a fertility examination with our fertility specialist.
Schedule a consultation appointment by contacting us at (021) 50200800 or chat with us via WhatsApp using the button below.
Mayo Clinic. [Last reviewed 16 Oct 2021]. Miscarriage. URL: https://www.mayoclinic.org/diseases-conditions/pregnancy-loss-miscarriage/symptoms-causes/syc-20354298.
After graduating from the Faculty of Medicine, University of Indonesia, dr. Fiona served as a Non-Permanent Employee (PTT) doctor from the Indonesian Ministry of Health in a remote village in Luwuk-Banggai Regency, Central Sulawesi. This experience led her to continue her master's degree in International Health at Gadjah Mada University, Yogyakarta.